Mental Health Services Overview
The Department of State Health Services (DSHS), which first owned and managed CMBHS, added functionality for mental health (MH) services in September 2013. CMBHS is now managed and supported by the Texas Health and Human Services Commission (HHSC) and the number and type of MH providers using CMBHS has increased.
This section of the CMBHS Help is to assist online MH services users to successfully navigate the system to find the information they need for service delivery, and to enter data for use by HHSC.
CMBHS Functions Available to Mental Health Services Users
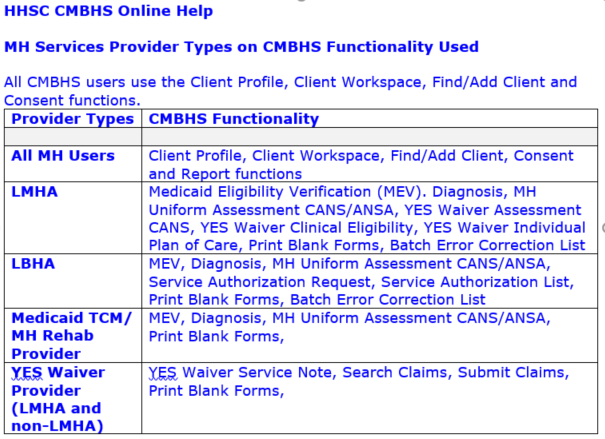
There are five mental health services provider types that use CMBHS.
When an MH services user logs in to CMBHS, the functions that display on the Administrative Toolbar (top) and the Client Services Toolbar (left) depend on the organization and location type designated by HHSC at setup.
See the following table for CMBHS functions available to each MH provider type.
Special Information for Mental Health Services Users
Billing and Claims – When using CMBHS for submitting claims to TMHP, have an Electronic Remittance Advice (ERA) form on file with TMHP. This form requests that TMHP create an electronic 835 file for your organization. Your organization (or another organization you specify such as a claims clearing house) must be designated on the form as the recipient of your 835 file. HHSC or DSHS may not be designated on the ERA as the recipient of the electronic 835 file.
Your organization may have already been contacted about this by TMHP and made the necessary changes; if not, contact the TMHP Contact Center: 1-888-925-9126 to verify the status of your ERA form.
TMHP places all electronic files at a secure FTP site. If you are interested in retrieving a file or files, call the TMHP Contact Center for instructions.
Episodes of Care (EOC) – Mental health services functions in CMBHS were designed to work in conjunction with the CARE data system. As a result, a data exchange process works nightly to ensure the data is synchronized.
The MH EOC begins with an Initial MH Uniform Assessment (CANS/ANSA) and ends with a Discharge MH Uniform Assessment (CANS/ANSA).
- The EOC rules limit a client to receiving services from one mental health provider at a time.
- When an MH client is in service with one provider, a second provider cannot access the Initial MH Uniform Assessment (CANS/ANSA) to obtain an authorization to provide the client additional services. (An MH Crisis Assessment is accessible.)
Data Exchange/Batching – At the time that CMBHS expanded to include mental health services, HHSC had an agreement with the Local Mental Health Authorities (LMHAs) to offer a data exchange process for every mental health function added to CMBHS. The LMHAs had electronic health records (EHR) to collect data and wanted to submit data to HHSC using the efficiency of a single data system rather than double entry. Data exchange requires that LMHAs first build the functionality in their EHR with CMBHS rules.
Limited provider and HHSC resources have checked the expansion of data exchange beyond the LMHAs and LBHAs.
View LMHA Network – LMHAs and Local Behavioral Health Authorities (LBHAs) are special types of mental health providers designated as local mental health authorites by the executive commissioner of the Health and Human Services Commission, as they are defined in the Texas Administrative Code in accordance with Texas Health and Safety Code, §533.035(a), https://texreg.sos.state.tx.us/public/readtac$ext.TacPagesl=R&app=9&p_dir=&p_rloc=&p_tloc=&p_ploc=&pg=1&p_tac=&ti=25&pt=1&ch=412&rl=321
The above Code provides LMHAs and LBHAs special responsibilities, as well as access to information needed to fulfill those responsibilities.
In CMBHS, employees can be permitted by LMHA/LBHAs to view all records in CMBHS for a client, without client consent. This is true even if the client is receiving services from another LMHA/LBHA. This ability does not extend to clients being served by a non-LMHA/LBHA MH provider, or by substance use disorder services.
Find/Add Client and Client Profile
The first two functions you will probably use if you log in to CMBHS are Find/Add Client and Client Profile. These functions work the same for all provider types.
CLICK ON one of the links below to go to Help information about that topic.
Client Profile for MH Users
There is no clinical or service delivery information in the CMBHS Client Profile. Persons authorized by the MH provider (given a CMBHS account with a role that allows access) can search for and view a Client Profile.
Before doing so, users must be sure to follow applicable laws, their contract with HHSC — or with another entity such as a Medicaid Managed Care Organization (MCO) — and their organization’s policies/procedures.
Client consent is not needed to search for a Client Profile in CMBHS (unless required by the provider’s procedures or other authority) but each CMBHS user must need to know client information in order to fulfill the user's job responsibilities. CMBHS will not display any client information to the provider, beyond the Client Profile, unless it is authorized by law or the client.
If you search CMBHS and find the client you are seeking, you can go to the Client Workspace and begin documenting. You can insert new documentation directly into the client’s record. If you do not find the client, you can add him/her to CMBHS.
NOTE: If you create a duplicate Client Profile, CMBHS may not be able to connect records from past or future services delivered to the client to the Client Profile you are creating. Avoid creating duplicate Client Profiles.
NOTE: If you create a Client Profile in CMBHS today and later today, you search for that same client, you must enter the Client’s CMBHS number, or the Client’s First Name, or the Client’s Last Name to find that client’s profile in CMBHS. All the other search methods will work the next day, but on the day the Client Profile is created, only the three fields noted above will produce results.
Mental Health Diagnosis
CMBHS requires that a valid mental health diagnosis be entered in the system before a mental health uniform assessment can be documented. The rules for entering a mental health diagnosis in CMBHS are similar to the rules for entering a diagnosis into the Client Assignment and Registration (CARE) system. If changes are needed after entering the diagnosis, you can enter changes for up to seven days. A new diagnosis document can be created at any time.
From a mental health provider location, after selecting a client, access the MH Diagnosis page by clicking on Diagnosis on the Client Services Toolbar at the left side of your screen.
Action Buttons on the Diagnosis
Action Buttons display in the top right and bottom right corners of the screen. The buttons that display depend on your role, location, the number of days since the last change to the document, document status, and whether the document is in View or Edit mode.
- When the diagnosis is within the seven day Edit/Delete time frame, and in EDIT mode, the following buttons will display: Save and Continue, Save, and Cancel.
- When the diagnosis is in view mode and the Document Status is in Draft, Ready for Review, or Closed Complete, the following buttons display: Edit, Close, Delete, and Print.
- When the diagnosis is past the Edit/Delete timeframe of seven days since the last document change, then the following buttons will display: Close, and Print.
Before You Start a Diagnosis
- Your organization must have a contract with HHSC or with a Medicaid managed care organization (MCO), or other approved agreement with HHSC, to use CMBHS and enter an MH diagnosis for a client.
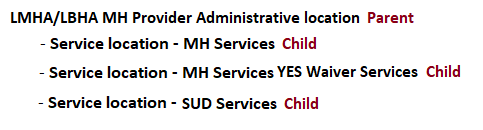
- Assessments are completed at the CMBHS service location level. Client services cannot be documented at the parent/administrative level of the organization.
- Click here for information about Roles according to Page Rights in CMBHS.
- You must be in the client’s CMBHS Health Record, at the Client Workspace, to document or view an MH diagnosis.
- The client must have a Client Profile in CMBHS before an MH diagnosis can be documented.
- Before you document in a client record, confirm that you have the record for the correct client by checking the client’s name and at least one other identifier at the top of the page. Correcting errors in CMBHS is time-consuming and can put confidential client data at risk.
General Rules for the MH Diagnosis
- A diagnosis can be entered for a person even if he/she has an open episode with another MH provider.
- An MH diagnosis can be documented for an MH client at any time, but is required annually.
- A diagnosis documented at an MH location cannot be used to meet requirements for diagnosis at a substance use disorder (SUD) treatment location. A diagnosis documented at a provider’s SUD location cannot be used to meet requirements for an MH diagnosis at an MH location.
- An MH diagnosis in any status can be edited or deleted at any time. If more than one MH diagnosis will be deleted, they can be deleted in any order.
- CMBHS allows editing and deletion of an MH diagnosis only by the provider that created it. Users cannot edit or delete an MH diagnosis created by another provider organization.
- An MH diagnosis may be deleted even when the MH diagnosis was used to fill the requirement for a valid MH diagnosis for documentation of an MH Uniform Assessment.
CAUTION: If an MH diagnosis is deleted or edited and there are dependent documents that have been created using that MH diagnosis, the client’s Level of Care and/or eligibility status may be negatively affected. The impact to the dependent documents may not be evident until the user tries to open or edit those documents.
MH Diagnosis Data Fields
Local Case Number (LCN) (Required)
- The LCN is a unique number assigned to a client by your agency. The LCN cannot be entered into this field, it must be entered in the Client Profile.
Instructions for Entering the Local Case Number (LCN) Local Case Number (LCN) into the Client Profile
- Go to the top of the page and click on the client's name in blue. The Client Profile will open in a pop-up box.
- Enter the LCN in the first tab.
- When the LCN is saved in the Client Profile, the LCN will automatically display in the LCN field of the Diagnosis and MH Assessment pages.
- If you have entered the LCN into the Client Profile, but it does not display in the LCN field of the MH Assessment, return to the Client Profile and use your web browser's refresh function.
Diagnosis Date (Required)
- Enter the date the diagnosis was made.
- The Diagnosis Date must be on or after the Client Profile Date.
- If the Diagnosis Date and the Client Profile Date are the same, the Diagnosis Time cannot be before the Client Profile time.
- CMBHS allows the creation of more than one diagnosis document on the same date if the Diagnosis Time is different for each.
- Enter the eight (8) numbers of the date (mmddyyyy) in the text box and CMBHS will put them in the correct date format. Or, you can enter the numbers and slashes (mm/dd/yyyy).
Diagnosis Time (Required)
- Enter the time the diagnosis was made.
- Enter the time in the text box by entering the four (4) numbers (hhmm) of the time and CMBHS will put them in the correct time format, or you can enter the numbers and the colon (hh:mm).
Documenting the Diagnosis
- The search method for diagnoses allows the user to type in a minimum of three characters associated with the code or a minimum of five characters associated with the diagnosis description, and the system will display all the codes related to the information typed in the row.
- Ensure that the diagnosis in the number one (1) slot is the diagnosis for which the client being treated. According to the Diagnostic and Statistical Manual of Mental Disorders (DSM 5), the diagnosis being treated is referred to as the Principal diagnosis and it should be first.
- The user may arrange the numbers next to each diagnosis line to change the order of the diagnoses.
- Up to 18 diagnoses may be entered in the diagnosis rows.
- After a diagnosis has been found and displays in the row, select a justification.
- After you have added a diagnosis or all the diagnoses, CLICK ON the Save button.
Diagnostic Justification (Optional)
- CLICK ON the option that describes the reason the diagnosis was selected.
- By client report
- By clinician observation
- By collateral report
- By history
- By impression
- By physician report
Comments (Optional)
- This text field is for additional diagnostic comments.
- CLICK IN the text box and TYPE in the information.
Intellectual and Developmental Disabilities
(IDD) Information
This section of the CMBHS diagnosis page is completed only for persons diagnosed with an intellectual and developmental disability (IDD).
Rules for completion of this section
- If the diagnosis is an IDD disorder, completion of IDD section is required.
- If the Principle diagnosis is an IDD disorder, then the Current ABL is a required field.
NOTE: Items below marked with a "§" have decode information in the CARE Reference Manual.
IDD Information
Current ABL §
- Identifies a person's current Adaptive Behavior Level (ABL).
- If the Principle diagnosis is on Axis II, then the Current ABL is a required field. If the Axis II diagnosis is a Personality Disorder diagnosis, completion of IDD data is not required.
Potential ABL §
- Identifies a person's potential adaptive behavior level.
AAMD Date §
- Date of the physician's examination in which the AAMD diagnoses were determined.
- TYPE in the (8) eight numbers of the date, mmddyyyy, and CMBHS will format the date, or TYPE in the numbers with the slash marks, mm/dd/yyyy.
- The AAMD Date field is optional. If a date is entered, then it must be the same as or earlier than Decision Date.
- TYPE in the (8) eight numbers of the date, mmddyyyy, and CMBHS will format the date, or TYPE in the numbers with the slash marks, mm/dd/yyyy.
Primary AAMD §
- Indicate a person's primary AAMD disorder, if one exists. For persons with an IDD disorder only.
Secondary AAMD §
- Indicate a person's secondary AAMD disorder, if one exists. For persons with an IDD only.
Tertiary AAMD §
- Diagnosis to indicate a person's tertiary AAMD disorder, if one exists. For persons with an IDD disorder only. See CARE Reference Manual for decoding.
Genetic §
- Indicate whether the person has a genetic defect.
Cranial Anomaly §
- Indicate whether the person has a cranial anomaly.
Perception §
- Indicate whether the person has a perception disorder.
Sensory Impairment §
- Indicate whether the person has a sensory impairment.
Convulsive Disorder §
- Indicate whether the person has a convulsive disorder.
Psychiatric Impairment §
- Indicate whether the person has a psychiatric impairment.
- Enter the two (2) digit code.
Motor Dysfunction Type §
- Indicate the person's motor dysfunction type. Select the appropriate type from the dropdown list.
Motor Dysfunction Location Type §
- Indicate the person's motor dysfunction location. Select the appropriate type from the dropdown list.
Motor Dysfunction Severity Type §
- Select the appropriate type from the dropdown list. Indicate the person's motor dysfunction severity.
IQ (Intelligence Quotient) Score (Optional) §
- A person's IQ score.
- The IQ Score, IQ Test Date, and IQ Test Type fields are optional. If a date is entered in one of those fields, however, the other two fields are required.
IQ (Intelligence Quotient) Test Date (Optional)
- Enter the date the SQ test was administered. The IQ Test Date cannot be later than the current date.
- TYPE in the (8) eight numbers of the date, mmddyyyy, and CMBHS will format the date, or TYPE in the numbers with the slash marks, mm/dd/yyyy.
IQ (Intelligence Quotient) Test Type
- Select the appropriate Type of IQ test from the dropdown list.
SQ (Social Quotient) Score § (Optional)
- Document the person's SQ score.
- The SQ Score, SQ Test Date, and SQ Test Type fields are optional. If a value is entered in one of those fields, however, then the other two fields are required.
SQ (Social Quotient) Test Date (Optional)
- Document the Date the SQ test was administered. The SQ Score, SQ Test Date, and SQ Test Type fields are optional. This field is required if either SQ Score or SQ Test Type is entered.
- The SQ Test Date cannot be later than current date and time.
- TYPE in the (8) eight numbers of the date, mmddyyyy, and CMBHS will format the date, or TYPE in the numbers with the slash marks, mm/dd/yyyy.
SQ (Social Quotient) Test Type (Optional)
- The SQ Score, SQ Test Date, and SQ Test Type fields are optional. This field is required if either SQ Score or SQ Test Date is entered.
- Select the appropriate type of SQ test administered from the dropdown list.
Document Status (Required)
- Select the appropriate Document Status and save.
- Draft
- Closed Complete
Document Status Date (System Generated)
- This date represents the date of the Document Status.
- The Document Status cannot be edited by the user.
What's Next?
- If you have not finished documenting all the information on the diagnosis page, select Draft from the Document Status dropdown list.
- If you are finished documenting the MH diagnosis, select Closed Complete from the Document Status dropdown list. CLICK on Save.